Summary by Jantima Tanboon, MD
Publication
N Engl J Med. 2022 Oct 6;387(14):1264-1278.
doi: 10.1056/NEJMoa2117912.
Trial of Intravenous Immune Globulin in Dermatomyositis.
Aggarwal R, Charles-Schoeman C, Schessl J, et al.
https://pubmed.ncbi.nlm.nih.gov/36198179/
Trial of Intravenous Immune Globulin in Dermatomyositis
One preparation of intravenous immune globulin (IVIG) has been approved by the US Food and Drug Administration (FDA) for the treatment of adult dermatomyositis (DM). This approval was based on the results of the Progress in Dermatomyositis (ProDERM) trial, the phase 3 randomized, placebo-controlled trial, recently published by Aggarwal R., et al.
The trial included 95 adult patients (age 18-80 years old) from 36 European and North American centers who were diagnosed with active DM according to Bohan and Peter criteria during 2017-2019 and met the following criteria: (1) prior treatment with a glucocorticoid or other immunosuppressive drug with either no response or an adverse event or currently receiving concomitant treatment with a glucocorticoid, a maximum of two immunosuppressive drugs, or both and (2) muscle weakness according to the manual muscle test-8 with at least 2 abnormal findings on the following 5 core measures: physician’s global assessment and patient’s global assessment disease activity; health assessment questionnaire; extramuscular disease activity; and serum muscle-enzyme levels.
The randomized phase was from week 0 to week 16 and the open-label extension phase was from week 16 to week 40. Any patient developed confirmed clinical deterioration at or after week 8 at two consecutive visits would be crossed over to the other trial group. Patients were allowed to continue into the open-label extension phase except for those who had clinical deterioration during IVIG trial. The primary end point was at least minimum response by Total Improvement Score (TIS, scores range 0-100 with higher score indicate greater improvement) at week 16 and no confirmed deterioration up to week 16.
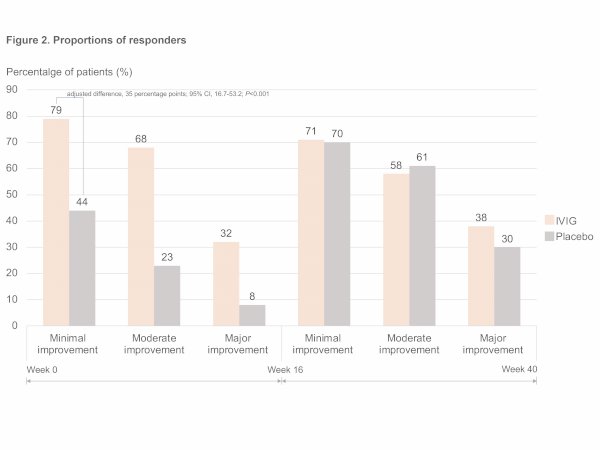
Among 95 eligible patients, 47 were assigned to the IVIG group and 48 to the placebo group (Figure 1). At week 16, a response of at least minimal improvement (TIS≥20) was observed in 79% (37/47) in the IVIG group and in 44% (21/48) in the placebo group (adjusted difference, 35 percentage points; 95% CI, 16.7-53.2; P<0.001). Percentages of patients with a response of at least moderate improvement (TIS ≥40) and a response of major improvement (TIS of ≥60) in the IVIG group were also higher. The TIS score in the IVIG group at week 16 was higher than the placebo group (47.7±24.2 vs. 21.3±20.8; 95% CI, 17.2-35.6).
At week 40, after open label extension phase, the percentages of patients who had at least minimal, at least moderate, and major improvement in both groups were virtually similar (Figure 2). Six serious IVIG-related thromboembolic adverse events and three non-thromboembolic adverse events (i.e. muscle spasm, dyspnea, and loss of consciousness) occurred during or within 72 hours after an infusion cycle during randomized and open-label extension phases.
Notably, although all the participants presented with typical DM rash and muscle weakness, myositis specific antibody (MSA) was not used to classify or confirm DM in the trial. This is likely because the ProDerm trial started before the current classification criteria for idiopathic inflammatory myopathies were available; the trial included 41 MSA positive patients and 20 myositis associated patients.
Among 41 patients with MSA, 49% (20/41) were positive for dermatomyositis-specific, 39% (16/41) antisynthetase, and 12% (5/41) immune-mediated necrotizing myopathy-associated antibodies. The heterogenous antibody subtypes, however, suggests possible IVIG responsiveness among different inflammatory myopathy subtypes.
Since the trial included adult patients with a combination of rash and muscle weakness, responsiveness in juvenile patients, patients with amyopathic dermatomyositis, and inflammatory myopathy patients without typical DM skin lesion require further evaluation. Further studies also need to explore the responsiveness to IVIG in different MSA subtypes and its efficacy beyond 16 weeks.
Dr. Aggarwal is a professor of medicine at University of Pittsburgh and medical director of Arthritis and Autoimmunity Center at University of Pittsburgh Medical Center. He is the co-director of UPMC Myositis Center. His research and clinical areas of interest are clinical and translational research in inflammatory muscle diseases (myositis) and associated interstitial lung disease. He is the past-chair of the medical advisory board of The Myositis Association (TMA) as well as past-chair of the scientific committee of IMACS, which are the largest patient and physician groups working in the field of myositis, respectively.
Dr. Aggarwal is an established independent clinical investigator with significant funding from NIH, foundations and industry and currently leading several collaborations internationally with other key leaders in the world. He has maintained an extremetly high publication record and recieved national and international recognition of his work. He continues to be a leader in disease criteria and outcomes measures in myositis as well as in clinical trials of novel therapeutic agents for myositis. He is currently the prinicipal investigator or member of the steering committee for several international phase 2/3 clinical trials in the area of myositis and associated ILD. Dr. Aggarwal is also mentoring future generation of rheumatologist with great success and attracting younger rheumatologist towards myositis research for the advancement of the field. Dr. Aggarwal lectures at various international conferences and promotes patient education through his YouTube channel.
This article is presented by the
Publication Highlights Committee.
Published on 23 January 2023.

16 Jan 2024 Anti-cN1A antibodies: epiphenomenon or pathogenic?

15 Nov 2023 Antisense oligonucleotide targeting DMPK in patients with myotonic dystrophy type 1: a multicentre, randomised, dose-escalation, placebo-controlled, p

15 Nov 2023 Mass spectrometry-based identification of new anti-Ly and known antisynthetase autoantibodies